The problem hypothesis
This study seeks to establish whether alcohol consumption has a direct effect on vision or whether it causes systemic diseases that will cause a vision problem. It also covers systemic diseases related to alcohol consumption in Saudi Arabia and globally.
Systemic effect of alcohol
Excess consumption of alcohol results in health and social issues. In addition to this, alcohol consumption also affects several body organs, such as the brain, heart, nervous and digestive systems, liver, and kidneys. However, we may not be familiar with all the systemic effects of alcohol on the body. Some of the systemic effects of alcohol on the body include the following areas.
Brain and central nervous system
Alcohol is a depressant. Consequently, it reduces activities of the central nervous system. It can cause drowsiness, and in some cases, excessive consumption has caused coma and deaths. Effects of alcohol consumption spread to motor functions and body reflexes. Prolonged consumption of alcohol results in poor reactions to different circumstances, mental conditions, and in worse cases, wet brain conditions or Korsakoff’s syndrome (permanent brain damage).
Parts of the brain, which are vulnerable to alcohol consumption, include the cerebral cortex. The cerebral cortex controls several brain functions, including decision-making and problem-solving abilities. Alcohol consumption also affects the hippocampus that controls memory and learning, and the cerebellum, which is responsible for movement coordination.
Studies have established links between alcohol consumption and its effects on vision (Alexander, 2002). This implies that consumption of alcohol can result in vision impairment. This is usually a distorted vision and inability to adjust to lights. Studies link alcoholism with red eyes and pinpoint pupils. Effects of alcohol consumption extend to other sense organs of the body such as ears, nose, and tongue.
Lungs
Alcohol abuse can cause significant weakness to the lungs. This makes the lung prone to health issues and other infections (pneumonia). Majorities who consume excess alcohol have suffered problems of breathing difficulties (alcohol poisoning), which may lead to deaths.
Liver
The liver suffers the most damage as a result of alcohol consumption. High contents of alcohol in the blood kill liver cells and inhibit the efficient operation of the liver. This condition causes liver cirrhosis. However, moderated consumption of alcohol allows the liver to repair the damaged cells.
Frequent and heavy alcohols consumption result in alcoholic hepatitis. This is a severe case of liver inflammation and cell damage. As a result, it leads to cirrhosis. Cirrhosis is an irreversible condition responsible for lesions, damage to liver cells, and scars. Such conditions may result in jaundice and edema. At the same time, damages to the liver may reduce blood clotting and cause liver failure, coma, and death.
Heart
Alcohol consumption can result in heart conditions related to “low ability to pump blood, weakening, abnormal heart signals, enlargement and irregular heartbeat” (Alexander, 2002). These conditions may result in heart failure. Alcoholism prevents the production of blood cells in the body. Alcohol addicts also neglect their diets resulting in weak bodies and insufficient vitamins and nutrients for the heart.
During Pregnancy
Health specialists warn pregnant women and breastfeeding mothers to refrain from alcohol consumption due to associated problems of alcohol consumption. Studies have established that consumption of alcohol during pregnancy can cause Fetal Alcohol Syndrome (FAS). Apart from FAS, there are also cases of stillbirths, miscarriage, low birth weight, defects, and premature births among others.
Any quantity of alcohol in the bloodstream of a pregnant woman passes on to the baby. Therefore, such contents of alcohol can cause harm to the baby’s physical and mental development and growth. Studies link FAS to “odd facial features, behavioral problems, learning disabilities and defects in the heart, lungs, bones, eyes, ears and the urinary tract” (Alexander, 2002).
Effects on Vision
According to Larry Alexander of John Kenyon Eye Centre, light alcohol consumption may not have any health problems. However, excessive consumption of alcohol may have systemic effects on the body including the eyes (Alexander, 2002). First, alcoholism leads to decreased visual performance. This is because heavy drinking affects normal brain function. It results in “weakened eye muscles causing blurred or double vision” (Alexander, 2002). There are also cases of “delayed eye reaction while driving” (Alexander, 2002). Second, alcohol consumption also causes reduced activities of the pupil due to its effects on constriction and dilation of the iris. Third, alcohol consumption also reduces the sensitivity of peripheral vision. This causes a condition of tunnel vision. Fourth, it also results in decreased contrast sensitivity. Thus, people may have difficulties identifying various shades of colour. Fifth, there is also a condition known as “optic neuropathy or tobacco-alcohol amblyopia” (Kesler and Pianka, 2003). This condition results from excessive smoking and drinking. Some health experts attribute this condition to toxic elements in alcohol and tobacco. Sixth, some specialists also link frequent migraines from alcohol consumption to temporary, debilitating visual aura just before the headache (Alexander, 2002). Finally, heavy drinking affects eye appearance as it results in eye redness. This is because of the expansion of the eye blood vessels.
Hiratsuka, Ono, and Murakami conducted research to establish a link between cataracts and alcoholism. They established inconsistent results between alcohol consumption and cataract. These researchers concluded that further research is necessary to identify such relationships (Hiratsuka, Ono and Murakami, 2009).
Shimozono and other researchers note that alcoholism affects “about 10 percent of men and 3 percent to 5 percent of women in their lifetime” (Shimozono et al, 1998). They observe that alcoholism relates to genetic, environmental, and psychosocial issues. These factors affect the development and manifestation of alcoholism. They reviewed acute vision loss that results from alcohol consumption and noted that such cases resulted from systemic diseases such as chronic anaemia, pancreatitis, and previous gastrojejunostomy and pancreatojejunostomy conditions the alcohol addict suffered. They noted that alcohol-induced nutritional optic neuropathy required effective management of the alcohol patient. In addition, they noted that the condition was treatable.
There is also toxic optic neuropathy related to alcohol abuse. Kesler and Pianka noted that the disease is complex and multifactorial. It resulted from “nutritional, toxicologic, environmental, and genetic factors” (Kesler and Pianka, 2003). These researchers related nutritional amblyopia to developing countries, though there were cases in developed nations. The researchers noted that cases of toxic amblyopia present in developed nations resulted from alcohol abuse. The condition is progressive leading to painless loss of visual from central or cecocentral scotoma. The disorder has no known specific remedy, but nutritional management and early detection can prevent severe consequences.
The spread of the problem worldwide and regionally (Saudi Arabia)
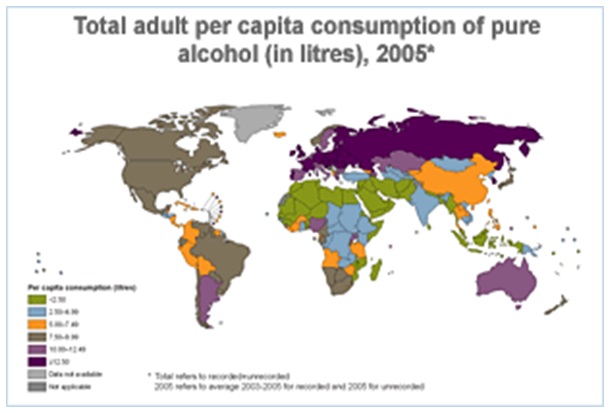
According to World Health Organisation Report 2011, at least 2.5 million people died from the harmful use of alcohol (WHO, 2011). The report associates at “least 60 different types of diseases to alcohol as it plays a significant causal role” (WHO, 2011). The report uses the GISAH indicator to monitor and assess health conditions and trends concerning “alcohol consumption, alcohol-related harm, and policy responses in countries” (WHO, 2011). This report also claims that unrecorded alcohol consumption accounts for “nearly 30 percent of the global total adult consumption” (WHO, 2011).
Source: WHO Report 2011.
Death rates of alcohol use disorders
Situation and trends, 2004. Source: WHO Report 2011.
Alcoholism in Saudi Arabia
The WHO does not have any data on alcohol consumption and its effects in Saudi Arabia (WHO, 2011). This is because the country has a total ban on alcohol. The country has strictly banned any production, importation, and consumption of alcohol-based on interpretations of the Koran. Consequently, any contact with alcohol has severe consequences. However, these strict regulations have not deterred people from brewing and consuming alcohol in Saudi Arabia (Hawwari, 2001).
Most alcohols in Saudi Arabia are homebrews from sugar and yeast. Foreigners also have their own brewing systems. Saudi diplomats and other foreigners usually import standard alcohol from other countries. However, this option is difficult for non-diplomats.
Saudi Arabia has no legal bars. Thus, most drinking places are usually in closed compounds. People mainly consume homebrew varieties at these informal gatherings.
Homebrews and Alcoholism in Saudi Arabia
Homebrews in the Kingdom have unknown alcohol strength. Thus, it is difficult for consumers to know what they are consuming. The popular homebrew is Sid. This spirit has up to 90 percent of alcohol content in addition to unknown impurities. Thus, alcohol poisoning is common in the Kingdom.
People who want to quit alcoholism usually accept contracts in Saudi Arabia. They tend to believe that the total ban on alcohol consumption can deny them access to alcohol. However, this is not the case due to the availability of homebrews. These homebrews are extremely lethal and have severe consequences on health.
The total ban of alcohol in Saudi Arabia implies that there are no existing options for addicts. Thus, addicts who need professional help must seek treatment outside the country. The lack of sufficient data on alcohol consumption, trends, and its effects in Saudi Arabia has complicated the situation. In addition, any addict prefers to remain unknown due to the stigma associated with alcoholism in Saudi Arabia.
The effect of the problem in the environment, population, and economy globally and regionally
Alcoholism has various adverse effects on society, economy and the work environment. Alcoholism affects many people other than the consumer alone. It affects the family in terms of providing health care during treatments.
In a social setting and work environment, alcoholism can result into absenteeism. This could be due to sick leave and other social issues. For instance, the WHO Report 2004 estimated that alcoholism contributed to 30 percent of absenteeism in Costa Rica (WHO, 2004).
Most countries strive to establish economic and social impacts of alcohol consumption at national levels. Studies concentrate on the negative effects of alcohol on social and economic costs. Alcohol consumption affects the social structures of societies. These include social behaviours and their related consequences. Economically, countries lose valuable workforce and resources to alcoholism. For instance, in Italy and Canada, the social and economic costs of alcohol are 5 to 1.1 percent of the Gross Domestic Product (GDP) respectively (WHO, 2004).
Information on the harmful effects of alcohol is useful in formulating public policies for regulating alcohol consumption and its effects. Such data also helps in the effective allocation of resources among competing health concerns. In addition, we can use such data to assess the effectiveness of implemented policies and identify information gaps. However, determining the social costs of alcohol remains difficult, but we can relate them to costs of care and other resources used to deal with alcohol.
This is significant for countries like Saudi Arabia, which have no data on alcohol production, distribution, and consumption as there are emerging trends of alcohol consumption with serious effects in the Kingdom.
Emerging trends: Blindness and alcohol consumption
There are emerging trends of blindness related to the consumption of illicit brews across the world, and Saudi Arabia has also reported such cases. For instance, in 2006, Khaleej Times reported that more than 20 people died after drinking laced cologne in Mecca while 40 people were in critical condition (Khaleej Times, 2006).
The poisoned cologne has serious health implications such as “migraines, nausea, vomiting, severe stomach and back pains and infection of the pancreas as well as malfunctions in the nervous and respiratory systems” (Khaleej Times, 2006). Since the country banned alcohol, some residents have turned to cologne as a replacement for alcohol.
Globally, such cases are rampant in Africa where people consume illicit brews. For instance, in Kenya over 140 people died in November 2000 after consuming illegal brews. Majorities went blind while hundreds survived after hospitalisation. This drink has unknown contents, but some of its lethal ingredients include methanol, formalin, and acid from car batteries (WHO, 2004).
These are some of the emerging trends in alcohol consumption, which health care providers must handle. The WHO reports these as “harmful consumption of alcohol, which accounts for 30 percent of the global consumption” (WHO, 2011).
Treatment
Most alcohol addicts are reluctant to seek treatment because they do not recognise their problems. Effective intervention from a professional can start the treatment process. Alcoholism has many treatments, but they depend on the severity of the case. In all, there are brief interventions, counselling programmes, and rehabilitation options with the aim of making the addict quit alcohol. Quitting alcohol is not a simple task for addicts and reducing consumption is not an effective approach. Thus, treatment should aim at eliminating alcohol consumption and enhancing the quality of life for the addict. Some of the treatment approaches may include detoxification and withdrawal, counselling, medication (Antabuse drugs), and treatment of other alcohol-related conditions (Fisher and Harrison, 2008).
Ethical problems
Alcohol research involves dealing with vulnerable populations, which may include even minors and cognitively impaired subjects. As a result, ethical issues may arise. Thus, research must observe conditions related to confidentiality of the research. However, the researcher must also recognise that other subjects not classified as vulnerable may also be vulnerable based on the terms of the research (Lowrance, 2003).
The researcher shall collect sensitive data from subjects. These data relate to alcohol and other substance abuse, reproductive data, age, economic status, and other background information about the subject. These pieces of information require confidentiality regardless of research situation or location.
Alcohol addicts may not agree to participate in research unless the researcher can guarantee complete confidentiality of information. Any other usage apart from research purposes or access by a third party needs written consent or knowledge of the subject.
Subjects have the right to privacy and can only provide information when the research shall keep Protected Health Information (PHI) confidential. However, as fields of study expand, maintaining confidentiality becomes complex. As a search, the researcher needs to be “extra vigilant so as not to lose the trust of the subjects and the public as Lowrance notes” (Lowrance, 2003).
Avoidance of ethical problems, through maintaining confidentiality, ensures that the researcher respects the subject, maintains the subject’s dignity and reduces cases of doubts among research participants.
Teams for the study
The team for the research shall consist of the primary researcher and his team. The process for conducting health research is demanding and time-consuming. This is because the researcher must interview subjects for the study. Later, the researcher must also determine their eligibility for the study. Patients expect the researcher to keep such information private especially if the researcher is not among the caregivers.
The primary researcher is responsible for information gathered from participants. Thus, the researcher must ensure that research assistants adhere to confidentiality and PHI requirements.
Conclusion
This research investigated whether alcohol has a direct effect on vision, or it causes systemic diseases that will cause a vision problem. The findings reveal that alcohol does not have a direct effect on vision. Instead, it affects the normal brain function, which later affects vision. At the same time, the research has also established that limited studies exist in this field. For instance, the WHO studies on harmful effects of alcohol consumption do not focus on the effects of alcohol on vision. Instead, the research in general and concentrates on deaths and other well-known diseases related to alcohol.
We have also established that Saudi Arabia has no existing record on the consumption of alcohol whether legal or illicit. This is because of a total ban on alcohol. However, there are emerging trends in the consumption of lethal homebrews with unknown contents in Mecca. Saudis have resorted to cologne laced with dangerous chemicals as substitutes for alcohol. This trend is also common in developing nations, and it comes with severe consequences of deaths and blindness. These are emerging challenges health care providers and policymakers must formulate strategies to handle.
Alcohol remains a deadly commodity to its consumers. It provides social and pleasure to its consumers. However, its effects remain severe and widespread.
The condition in Saudi Arabia shows that alcohol policies should be specific to regions. The country should establish its studies on volume and patterns of consumption in the area so as to reduce the lethal effects of alcohol. Consequently, countries must adopt national alcohol monitoring systems in order to assist in identifying consumption patterns and dangerous effects of alcohol. This is important for creating awareness among the concerned parties. However, controlling alcoholism requires cooperation between the government and the public during the formulation of policies.
The social and economic costs of alcoholism affect the lives and communities of the addicts. The worrying trends are escalating deaths and increasing consumption of harmful alcohol across the globe.
References
Alexander, L. (2002). Primary Care of the Posterior Segment (3rd ed.). New York: McGraw-Hill Medical.
Fisher, G. and Harrison, T. (2008). Substance Abuse: Information for School Counselors, Social Workers, Therapists, and Counselors (4th ed.). London: Allyn & Bacon.
Hawwari, A. (2001). Getting a drink in Saudi Arabia. Web.
Hiratsuka, Y., Ono, K. and Murakami, A. (2009). Alcohol use and cataract. Curr Drug Abuse Rev., 2(3), 226-9.
Kesler, A. and Pianka, P. (2003). Toxic optic neuropathy. Curr Neurol Neurosci Rep., 3(5), 410-4.
Khaleej Times. (2006). Pour me a glass of your finest eau de toilette. Mecca: Khaleej Times.
Lowrance, W. (2003). Learning from experience: Privacy and the secondary use of data in health research. J Biolaw Bus., 6(4), 45.
Shimozono, M., Townsend, C., Ilsen, F. and Bright, C. (1998). Acute vision loss resulting from complications of ethanol abuse. J Am Optom Assoc., 69(5), 293- 303.
WHO. (2011). Global Information System on Alcohol and Health (GISAH). Web.
WHO. (2004). Global Status Report on Alcohol 2004. New York: WHO.